
Support
Be her support when she feels unsure
45% of pregnancies and 1/3 of births in the UK are unplanned or associated with feelings of ambivalence1
50% of women (18-35) have had unprotected sexual intercourse (UPSI) in the past year 2
25% of unintended pregnancies ended in abortion 3
Between Jan 2022 - Jun 2022 UK abortions increased by 17% compared to 2021 4
- Pharmacy
2nd most trusted source of healthcare guidance amongst consumers(after nurses) 5

Ensure your pharmacy team have read the SmPC for both ellaOne® and Hana® to be the best support she needs.
Comfort
Be her comfort when she needs reassurance
When choosing emergency hormonal contraception (EHC) the most important factors that influence a person’s decision are:
Effectiveness
84% of women rate effectiveness as the most important factor when buying EHC.8
Pharmacist Recommendation
Pharmacy recommendation is the second most important factor 8. However, if a woman doesn’t understand that ellaOne® is the most effective EHC, she will ask generically for ‘the Morning After Pill’ and seek your recommendation.
Price is the least important factor.8In fact, 83% of women would be willing to pay more for a more effective product. 9
Why is ellaOne® more effective?
Pregnancy rates per 1000 women in the first 24 hours after unprotected sex 10*
-
55 with no intervention**
-
23 with levonorgestrel
-
9 with ellaOne®
ellaOne® is 2.5 x more effective than levonorgestrel 10
*Meta-analysis of two comparative randomised, non-inferiority trials involving 1184 women receiving emergency hormonal contraception within 24 hours of unprotected sexual intercourse **Estimated.
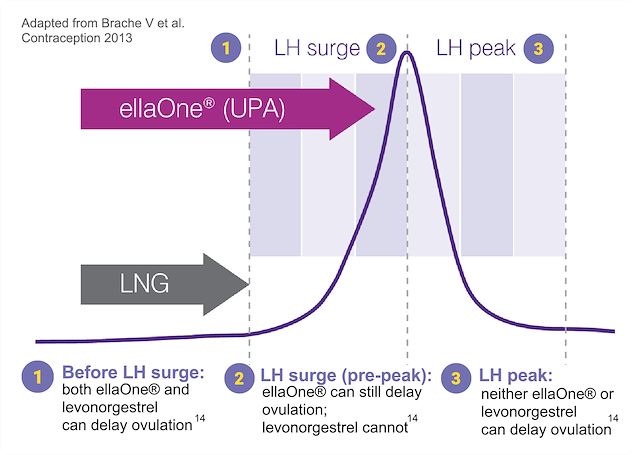
Only ellaOne® works on the most fertile days just before ovulation (during the Luteinising hormone surge).12
Remember: ovulation is unpredictable. 88% of women do not ovulate on day 14.13
FSRH logo The latest national emergency hormonal contraception (EHC) guidance from the FSRH recommends ‘Pharmacists should consider ulipristal acetate (ellaOne®) as their first line recommendation in EHC.14
The new "Be Her..." training materials
These include: interactive emergency contraception consultation tool, co-branded ellaOne® & Hana® training guide and window sticker.


Use of these materials is optional, and you should use your professional judgement to decide when and how to use them.
Solution
Be her solution when she wants convenience
28 % of women change their method of contraception after having unprotected sex 15
Offering a 3-month supply of Hana® to customers buying emergency contraception can lead to more effective contraception use, so you can be confident in discussing Hana® with women buying ellaOne® 16
NICE guidance recommends providing at least a 3-month supply when starting a woman on a POP 17
This helps improve compliance and allows more time for the woman to adjust to her new method and bleed profile to settle.

How does it work?
Hana® prevents pregnancy in two independent ways:
Why Hana?
No other contraceptive pill is more effective than Hana® 21it contains the progestogen desogestrel which is over 99% effective when used correctly 22
The UK’s best selling OTC daily contraceptive pill in pharmacy 23
It’s suitable for many women 2224, including those breastfeeding and women who are unable to use oestrogens or prefer not to.
Guidance
Be her guidance when she feels lost
For some customers, just starting the conversation can be a barrier when seeking advice.
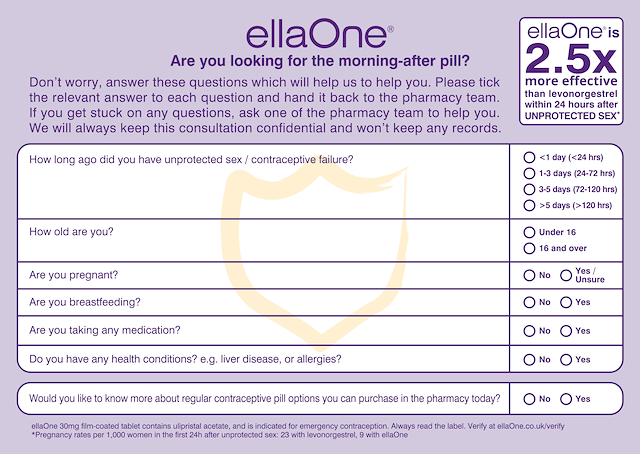
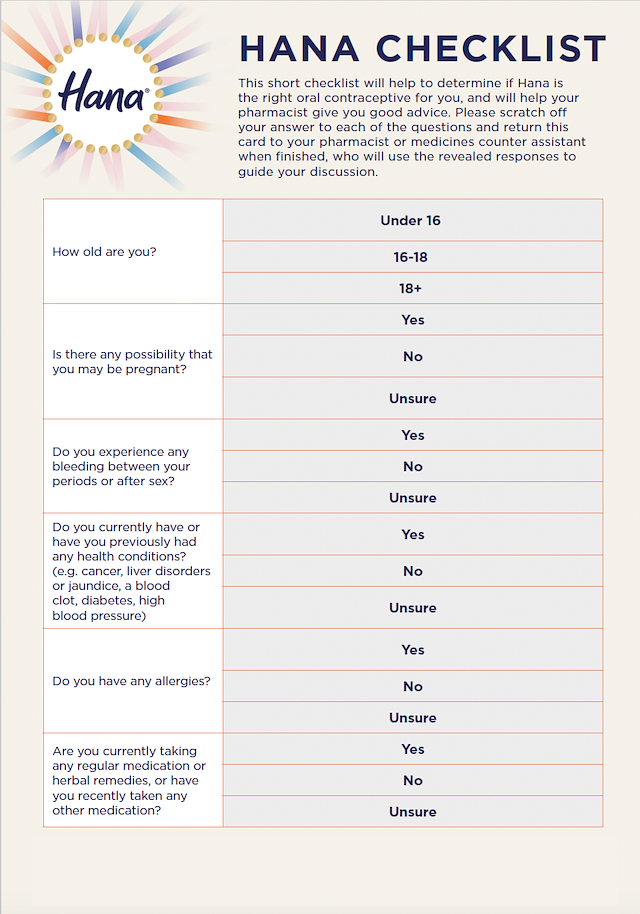
To meet the needs of ellaOne® and Hana®, we have created two separate Consultation Checklists:
These allow women to discreetly answer a few simple questions about their health and needs
They are also designed to assist in your consultations, allowing you to check their suitability and provide appropriate advice
The ellaOne® checklist features a new question to determine if women would like to know more about regular contraceptive pills they can purchase in pharmacy, as the perfect introduction to discuss Hana®.
72 % of women stated they would like to use a card like the EC checklist 25
Need additional ellaOne® and/or Hana® Consultation Checklists pads?
Use of these materials is optional, and you should use your professional judgment to decide when and how to use them.
Answers
Be her answers when she has questions
Knowing the correct information about emergency and regular contraceptive pills helps women make an informed decision about what’s most suitable for them.
Below are FIVE questions asked about ellaOne® and Hana® and our recommended answers. For advanced training, we have produced NPA-accredited, award-winning training including pharmacy support materials. Use the links below to access and ensure your pharmacy team is up to date in their knowledge and confident in their recommendations.
Pharmacy
Be her pharmacy when she needs you most
How you interact with your customers at a difficult time for them can set the template for future interactions as they continue their women’s health journey. Being their support, reassurance, and answers can also lay the foundation for you being her trusted healthcare partner.
The following are a few steps you can take:
Ensure ellaOne® and Hana® packs are visible on shelves behind the pharmacy counter - to help normalise and remove stigma from these categories
Use available point of sale materials both around the pharmacy and in consultation areas
Ensure all staff in your pharmacy are trained and equipped with the latest information and materials. This includes awareness of the use of both ellaOne® and Hana® checklists for customer discussions
Use positive, supportive language when discussing daily and emergency contraception with women
Below are a few examples of supportive language you can use:
ellaOne® and Hana® are supported by a £4M combined media campaign including Social and PR to encourage women to visit their pharmacy and discuss their contraception options with you.
Essential
Essential Information
PRODUCT INFORMATION ellaOne® 30 mg film-coated tablet (ulipristal acetate). Refer to the SmPC for further information. INDICATION: Emergency contraception (EC) within 120 hours (5 days) of unprotected sexual intercourse or contraceptive failure. DOSAGE: one 30mg tablet taken orally as soon as possible, but no later than 120 hours (5 days) after unprotected intercourse or contraceptive failure. Another tablet should be taken if vomiting occurs within 3 hours of intake. Can be taken at any time during the menstrual cycle. Not recommended for women with severe hepatic impairment. CONTRAINDICATIONS: Hypersensitivity to the active substance or excipients. SPECIAL WARNINGS AND PRECAUTIONS: Occasional use only. Use reliable barrier method after use until next menstrual period. If next menstrual period is delayed >7 days or is abnormal or suggestive symptoms occur then perform pregnancy test. Consider ectopic pregnancy. If pregnancy confirmed, woman should contact their doctor. Concomitant use with EC containing levonorgestrel not recommended. Does not contraindicate the continued use of regular hormonal contraception but reliable barrier method should be used until next menstrual period. Not recommended in severe asthma treated by oral corticosteroids. Concomitant use of CYP3A4 inducers [e.g. barbiturates (including primidone and phenobarbital), phenytoin, fosphenytoin, carbamazepine, oxcarbazepine, herbal medicines containing Hypericum perforatum (St. John’s wort), rifampicin, rifabutin, griseofulvin, efavirenz, nevirapine] not recommended (may decrease efficacy of ellaOne). Long term use of ritonavir not recommended. Not recommended for women who have used enzyme-inducing drugs in the past 4 weeks. Non-hormonal emergency contraception (i.e. a copper intrauterine device (Cu-IUD)) should be considered. Contains lactose. FERTILITY, PREGNANCY AND LACTATION: Not intended for use during existing or suspected pregnancy. Limited human data does not suggest safety concern. Does not interrupt existing pregnancy. No teratogenic potential was observed; animal data insufficient with regard to reproduction toxicity. Marketing Authorisation Holder maintains a pregnancy registry (www.hra-pregnancy-registry.com) to monitor outcomes of pregnancy in women exposed to ellaOne®. Patients and health care providers are encouraged to report any exposure. Ulipristal acetate is excreted in human breast milk; breastfeeding is not recommended for one week after intake. Breast milk should be expressed and discarded. A rapid return of fertility is likely following ellaOne use; regular contraception should be continued or initiated as soon as possible; subsequent acts of intercourse should be protected by reliable barrier method until next menstrual period. UNDESIRABLE EFFECTS: Always consult the SmPC before prescribing. Only the most common side effects and those which are rare but may be serious are listed below. Most commonly reported adverse reactions: headache, nausea, abdominal pain and dysmenorrhea. Common (≥1/100 to <1/10): mood disorders, dizziness, abdominal pain upper, vomiting, abdominal discomfort, myalgia, back pain, dysmenorrhea, pelvic pain, breast tenderness and fatigue. Rare (≥1/10,000 to <1/1,000): ruptured ovarian cyst. Hypersensitivity reactions including rash, urticaria, angioedema RETAIL PRICE: ellaOne 30 mg single film-coated tablet blister pack; £34.95.
MARKETING AUTHORISATION HOLDER Laboratoire HRA Pharma, 200 avenue de Paris, 92320 Châtillon, France. Marketed in the UK by: HRA Pharma a Perrigo Company, One Embassy Gardens, Viaduct Gardens, Nine Elms, London SW11 7BW, United Kingdom MARKETING AUTHORISATION NUMBER(S): PLGB 17836/0011. LEGAL CATEGORY: P
Date of last revision of text: October 2024
PRODUCT INFORMATION Hana 75 microgram film coated tablets (desogestrel). Indication: Hana 75 microgram film coated tablets contains desogestrel and is indicated for oral contraception in women of childbearing age to prevent pregnancy. Refer to SmPC for further product information. Dosage and Administration: One tablet taken orally. Must be taken at same time every day, always 24h interval between 2 tablets. First tablet should be taken on day 1 of menstrual bleeding, can be started on days 2-5, but barrier method recommended for first 7 days of tablet-taking. Thereafter one tablet daily (continuously) without taking any notice of possible bleeding. When pack of pills is finished, a new pack should be started directly the day after the previous one. Pre-existing bleeding abnormalities such as oligomenorrhoea and amenorrhoea should be investigated before starting Hana. Refer to SmPC for full directions on how to prevent pregnancy. Contraindications: Known or suspected sex-steroid sensitive malignancies. Women with breast cancer. Active venous thromboembolic disorder. Presence or history of severe hepatic disease (as long as liver function values have not returned to normal). Undiagnosed vaginal bleeding. Hypersensitivity to the active substance or excipients. Special warnings and Precautions: Exclude pregnancy before starting Hana. Before starting Hana, use reliable contraceptive method until first day of next period. Women should be advised if menstrual period does not come when expected, she may be pregnant, to do a pregnancy test or see a physician. Provided pregnancy test is negative she can start Hana on the first day of next period. Before starting a new pack of Hana, a woman should be certain she is not pregnant. Refer to SmPC for full directions. Refer to physician if any of the following conditions/risk factors are present: breast cancer, hepatic disorders and disturbances of liver function, hypertension, thromboembolic disorders, changes in bleeding patterns, diabetes, psychiatric disorders, ectopic pregnancy, effect on bone mineral density, conditions reported during pregnancy or during sex steroid use, chloasma, reduced efficacy in event of missed tablets, does not protect against HIV (AIDS) or other sexually transmitted infections, contains lactose, refer to SmPC for full warning and precaution information. Interactions: refer to SmPC for full interaction information. Undesirable Effects: Always consult the SmPC before prescribing. Only the most common side effects and those which are rare but may be serious are listed below. Most commonly reported adverse reactions: bleeding irregularity headache, acne, mood changes, depressed mood, decreased libido, breast pain, nausea and weight increase, amenorrhoea, irregular menstruation. Rare: rash, urticaria, erythema nodosum. On rare occasions ectopic pregnancies reported, hypersensitivity reactions, breast discharge can occur. Aggravation of angioedema and/or aggravation of hereditary angioedema may occur. In women using combined oral contraceptives a number of (serious) undesirable effects have been reported: venous thromboembolic disorders, arterial thromboembolic disorders, hormone-dependent tumours (e.g. liver tumours, breast cancer), and chloasma, breakthrough bleeding and/or contraceptive failure may result from interactions of other drugs (enzyme inducers) with hormonal contraceptives. Consult the SmPC in relation to other adverse reactions. Pack size: 28 tablets. Retail Price: £9.48 (1x28) £20.90 (3x28).
MARKETING AUTHORISATION Holder: Laboratoire HRA Pharma, 200 avenue de Paris, 92320 Chatillon, France. Marketed by: HRA Pharma a Perrigo Company, One Embassy Gardens, Viaduct Gardens, Nine Elms, London SW11 7BW, United Kingdom. MARKETING AUTHORISATION6 Number: PL 17836/0015. Legal Category: P Additional information and full Product Information is available on request from UKLOCustomerService@perrigo.com
Date of last revision of text: October 2024
Adverse events should be reported. Reporting forms can be found at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to HRA Pharma on 0203 598 9603 or email UKLOCustomerService@perrigo.com
References
References
- Health matters: reproductive health and pregnancy planning. Available at https://www.gov.uk/government/publications/health-matters-reproductive-health-and-pregnancy-planning/health-matters-reproductive-health-and-pregnancy-planning. June 2018 [Accessed November 2023]
- HRA data on file: ellaOne® Brand Performance Tracker, 1000 women aged 18-35, November 2022.
- Abortion statistics, England and Wales: 2021. Available at https://www.gov.uk/ government/statistics/abortion-statistics-for-england-and-wales-2021/abortion-statistics-england-and-wales-2021 [Accessed November 2023]
- Abortion statistics for England and Wales: England and Wales: January to June 2022. Available at https://www.gov.uk/government/statistics/abortion-statistics-for-england-and-wales-january-to-june-2022/abortion-statistics-for-england-and-wales-january-to-june-2022 [Accessed November 2023]
- 2023 Edelman Trust Barometer Special Report: Trust and Health. Available at https://www.edelman.com/sites/g/files/aatuss191/files/2023-04/2023/Edelman/Trust/Barometer/Trust/and/Health1.pdf [Accessed November 2023]
- Office for National Statistics (ONS). Estimates of the population for the UK, England and Wales, Scotland and Northern Ireland. February 2022 (mid-2020 dataset). Available at https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland [Accessed November 2023]
- HRA Pharma. Data on file 2020.
- HRA Data on file. Questionnaire of a representative sample of 700 sexually active UK women ages 16-45, 2013.
- HRA data on file. Consumer Research 2016. Festival Questionnaire of 933 UK women aged 18+.
- Glasier A et al. Lancet 2010; 375(9714):555-62.
- HRA data on file. HRA Pharma Report, Women and EC in 2012, a European survey of 7170 sexually active women aged 16-46.
- Brache V et al. Contraception 2013; 88; 611-618.
- Wilcox AJ et al. BMJ 2000; 321: 1259-62.
- FSRH Emergency Contraception CEU Clinical Guidance Document March 2023. Available at: https://www.fsrh.org/documents/ceu-clinical-guidance-emergency-contraception-march-2017/ [Accessed November 2023]
- IPSOS Field Research (Feb 2024), Growing Hana Brand in UK, March 2024 Report.
- Cameron, ST et al Lancet 2020 Nov 14:396(10262):1585-1594.
- NICE scenario: Progestogen-only pill, March 2021.
- Rice C, Killick S, Hickling D, et al. Ovarian activity and vaginal bleeding patterns with a desogestrel-only preparation at three different doses. Hum Reprod 1996;11(4):737- 740.
- Rice CF, Killick SR, Dieben T, et al. A comparison of the inhibition of ovulation achieved by desogestrel 75 micrograms and levonorgestrel 30 micrograms daily. Hum Reprod 1999;14(4): 982-985.
- McCann MF and Potter LS. Progestin-only oral contraception: a comprehensive review. Contraception 1994;50(6 Suppl 1):S1-S95.
- Faculty of Sexual & Reproductive Health Quick Starting Contraception Guidance 2017.
- Faculty of Sexual & Reproductive Healthcare Clinical Guidance (FSRH). Progestogen-only Pills. March 2015 (amended April 2019). Available at https://www.fsrh.org/standards-and-guidance/documents/cec-ceu-guidance-pop-mar-2015/ [Accessed November 2023].
- IRI data 19.03.22.
- Faculty of Sexual & Reproductive Healthcare Clinical Guidance (FSRH). UK Medical Eligibility Criteria for Contraceptive Use. April 2016 (amended October 2019). Available at https://www.fsrh.org/standards-and-guidance/documents/ukmec-2016/. [Accessed: November 2023]
- HRA Pharma Data on File: Consumer Research 2018. Festival Questionnaire of 750 UK women aged 18+. 26. Perrigo Women’s Health Data on File. 2023.